A. Cavezzi
pag. 26 Abstract Book of the 17th Congress
of the European Society of Phlebectomy
Geneve 1997
Varicosities of lower limbs (i.e. reticular varices and telangiectasias) are still characterized by haemodynamic patterns that are not completely clear. Saphenous insufficiency is being more and more closely investigated, in order to clarify the haemodynamic aspects of the refluxes, or of the downstream flows. Starting from the saphenous haemodynamic models, recent studies are trying to extend the knowledge of the superficial venous system pathophysiology to the smallest veins.
By means of several echo-colour-doppler examinations carried out during the last 6 years, we have studied the complex venous haemodynamics in all those patients presenting varicose veins of the lower limbs.
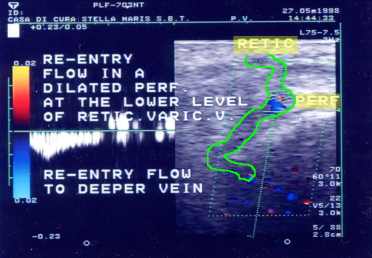
From the anatomical point of view, it is known that the superficial tiny venous vessels (capillaries) normally drain into the deeper reticular veins, which may finally join the tributaries of the main venous axes (saphenous and extra-saphenous ones); the superficial network, of course, may also reach the deep venous system (DVS) via perforating veins (PV). Anyway most of the PV seem to play a re-entry role into the DVS, directly or indirectly, having a little relevance to a superficial venous insufficiency (even when enlarged, the balance between drainage in the DVS and reflux into the superficial venous system is largely in favour of the former).
Using echo-colour-doppler exam we have studied many different patterns of varicosities, collecting several different findings, also dependent on limb position, the muscle contraction, their localization etc.
The lateral thigh plexus is usually characterized by the drainage of the telangiectasias in a reticular vein, which finally empties into a leg (or occasionally thigh) re-entry PV. Isolated bleb of telangiectasias may equally have a small underlying drainage venule. Saphenous refluxes can anyway transfer the ambulatory venous hypertension up to the visible superficial reticular and dermal varices. Many telangiectasias do not feature any specific connection with larger veins, e.g. in the trochanteric region. Finally, according to our experience the telangiectatic matting after surgery or sclerotherapy (as unpleasant as unexpectable), is sometimes an expression of haemodynamic difficulty, due to the abolished venous drainage into the avulsed or sclerosed ectasic vein.
Some of these echo-colour-doppler findings can vary according to the supine, raised or orthostatic position of the limb, as the influence of the orthodynamism is still ambiguous and difficult to investigate. For example, may we hypothisize in most patients a kind of mechanical "obstructed venous discharge syndrome" for the lateral thigh varicosities system during ambulation ? Do telangiectasias often originate before, affecting the reticular veins afterwards (as seems the case in saphenous tributaries disease, followed by trunk and junction reflux later...) ? Are the old fashion "feeding veins" always drainage veins ?
All these questions are the subject of discussion of this presentation, debating whenever possible the relative therapeutic implications concerning phlebectomy and sclerotherapy.
 Go Back |
 Home Page |
to the top |